+86-28-82633987sales@biopurify.com


EtoposideCAS No.:33419-42-0
|
||||||||||
 |
|
|
||||||||
| Catalogue No.: | BP3729 |
| Formula: | C16H18O4 |
| Mol Weight: | 274.31 |
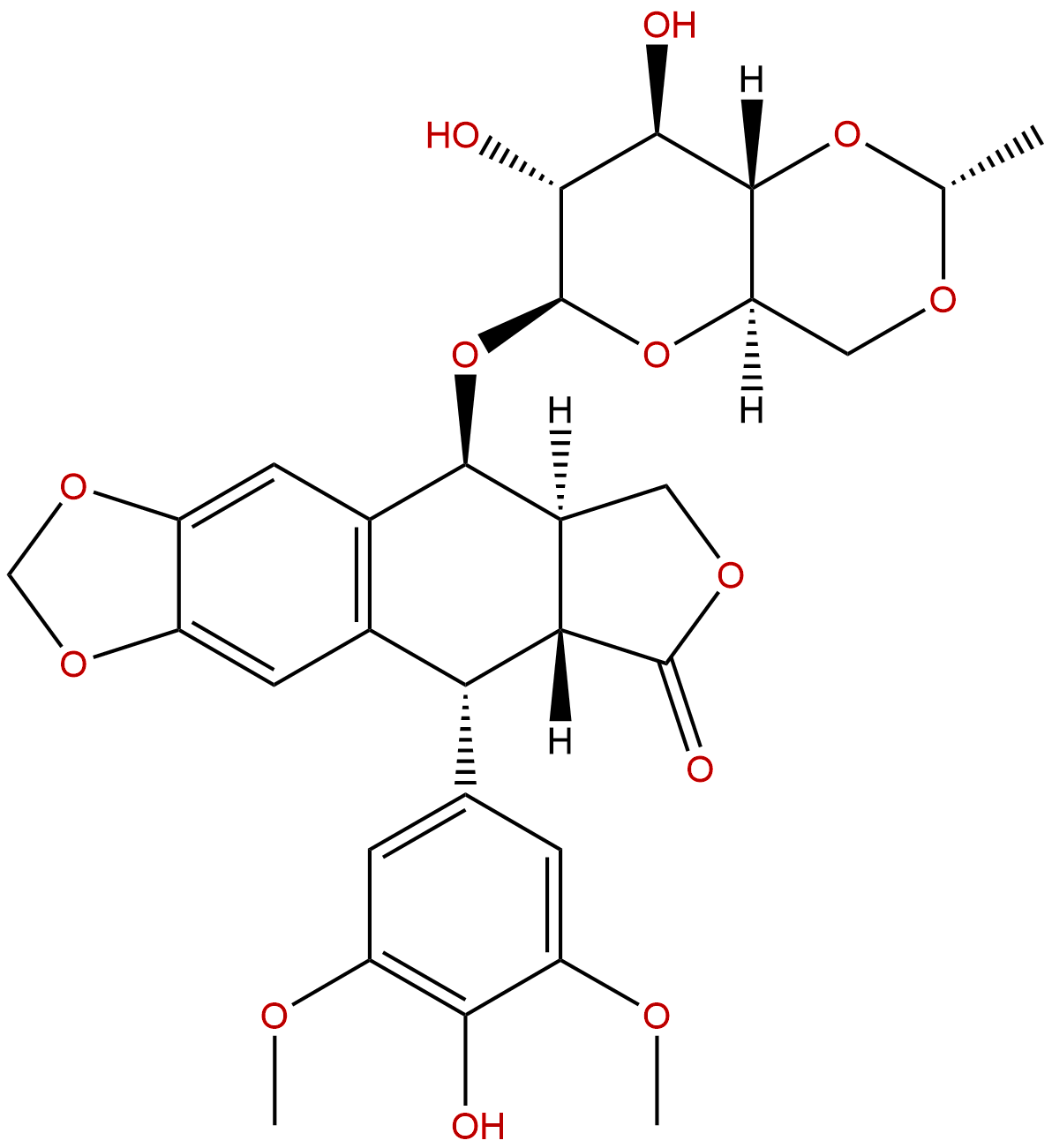
Product name: Etoposide
Synonym name: Etopl; Vepeside
Catalogue No.: BP3729
Cas No.: 33419-42-0
Formula: C29H32O13
Mol Weight: 588.562
Botanical Source:
Physical Description:
Type of Compound:
Purity: 95%~99%
Analysis Method: HPLC-DAD or/and HPLC-ELSD
Identification Method: Mass, NMR
Packing: Brown vial or HDPE plastic bottle
The product could be supplied from milligrams to grams. Inquire for bulk scale.
We provide solution to improve the water-solubility of compounds, thereby facilitating the variety of activity tests and clinic uses.
For Reference Standard and R&D, Not for Human Use Directly.
Description:
Etoposide is a chemotherapy medication used for the treatments of a number of types of cancer. Etoposide inhibits DNA synthesis by forming a complex with topoisomerase II and DNA, it induces apoptosis in MCF-7 breast cancer cells.
References:
Cancer Res. 2001 Jan 1;61(1):348-54.
Reconstitution of caspase 3 sensitizes MCF-7 breast cancer cells to doxorubicin- and etoposide-induced apoptosis.
MCF-7, a breast cancer-derived cell line, is deficient of caspase 3 and relatively insensitive to many chemotherapeutic agents.
METHODS AND RESULTS:
To study the association of caspase 3 deficiency and chemotherapeutic resistance, we reconstituted caspase 3 in MCF-7 cells and characterized their apoptotic response to doxorubicin and Etoposide. Western blots demonstrated that caspase 3 was constitutively expressed in the reconstituted MCF-7 cells. Both morphological observation and survival assays showed that caspase 3 reconstitution significantly sensitized MCF-7 cells to both drugs. Remarkably increased activation of caspases 3, 6, and 7, cleavage of cellular death substrates, and DNA fragmentation were detected in the reconstituted MCF-7 cells after drug treatment.
CONCLUSIONS:
Together, these data demonstrated a specific role for caspase 3 in chemotherapy-induced apoptosis and in activation of caspases 6 and 7. Our results also suggest that caspase 3 deficiency may contribute to chemotherapeutic resistance in breast cancer.
Endocr Relat Cancer. 2005 Sep;12(3):657-66.Etoposide, doxorubicin and cisplatin plus mitotane in the treatment of advanced adrenocortical carcinoma: a large prospective phase II trial.
METHODS AND RESULTS:
To investigate the activity of Etoposide, doxorubicin, and cisplatin plus mitotane in the management of advanced adrenocortical carcinoma (ACC) patients, 72 patients with measurable disease not amenable to radical surgery were enrolled in a prospective, multicenter phase II trial. EDP schedule (Etoposide 100 mg/m(2) on days 5-7, doxorubicin 20 mg/m(2) on days 1 and 8, and cisplatin 40 mg/m(2) on days 1 and 9) was administered intravenously every 4 weeks. Concomitantly, patients were given up to 4 g/day of oral mitotane. Five patients achieved a complete response and 30 a partial response, for an overall response rate of 48.6% (95% CI: 37.1-60.3). Median time to progression in responding patients was 18 months. The EDP regimen was well tolerated, leukopenia being the dose limiting toxicity. One toxic related death due to septic shock, however, was registered. Radical surgical resection of residual disease after chemotherapy was performed in 10 patients. The overall survival of patients attaining a disease free status (clinical complete responders+radically resected) was significantly higher than that of patients with partial response or no response (P<0.002). Androgen secretion was associated with long survival, while glucocorticoid secretion was associated with poor prognosis both in univariate and multivariate analysis.
CONCLUSIONS:
In conclusion, EDP plus mitotane is an active and manageable combination scheme for ACC patients. Surgical resection of residual disease subsequent to chemotherapy leads to a more favourable outcome. The natural history of the disease is significantly influenced by the secretory status of the tumor.J Clin Oncol. 2000 Mar;18(6):1173-80.Sequential dose-intensive paclitaxel, ifosfamide, carboplatin, and etoposide salvage therapy for germ cell tumor patients.
To evaluate the efficacy and toxicity of sequential, dose-intensified chemotherapy with paclitaxel/ifosfamide and carboplatin/Etoposide administered plus peripheral blood-derived stem-cell (PBSC) support for patients with germ cell tumors (GCT) who have unfavorable prognostic features in response to conventional-dose salvage programs. Carboplatin was dose escalated by target area under the curve (AUC; in [milligrams per milliliter] x minutes) among patient cohorts, and pharmacokinetic studies were performed for comparison.
METHODS AND RESULTS:
Thirty-seven previously treated patients who had cisplatin-resistant GCT and unfavorable prognostic features for response to conventional-dose salvage therapy were treated. Two cycles of paclitaxel 200 mg/m(2) plus ifosfamide 6 g/m(2) were given 2 weeks apart with leukapheresis, followed by three cycles of carboplatin plus Etoposide given 14 to 21 days apart with reinfusion of PBSCs. The dose of Etoposide was 1, 200 mg/m(2), and the carboplatin target AUC ranged among cohorts from 12 to 32 (mg/mL) x min. Pharmacokinetic studies of carboplatin were performed for comparison of target to measured AUC. Twenty-one patients (57%) achieved a complete response and an additional two patients (5%) achieved a partial response with normal tumor markers; therefore, 23 (62%) achieved a favorable response. Eight patients relapsed, and 15 (41%) of the favorable responses remained durable at a median follow-up of 30 months. Myelosuppression was the major toxicity; 58% of carboplatin/Etoposide cycles were associated with hospitalization for nadir fever. The AUC of carboplatin measured in serum was lower than the target AUC; this may be related to underestimation of the glomerular filtration rate used in the dosing formula.
CONCLUSIONS:
Dose-intense therapy with sequential, accelerated chemotherapy of paclitaxel/ifosfamide and carboplatin/Etoposide administered with PBSC support was relatively well tolerated. The durable complete response proportion was substantial in patients with unfavorable prognostic features for achieving durable complete response to conventional-dose salvage programs. Optimal dosing of carboplatin in the high-dose setting warrants further investigation.Leuk Lymphoma. 1994 Sep;15(1-2):127-30.Idarubicin, high-dose cytarabine and etoposide for remission induction in therapy-related acute myeloid leukemia
METHODS AND RESULTS:
Five patients with therapy-related acute myeloid leukemia received combination induction chemotherapy with idarubicin, high-dose cytarabine, and Etoposide. Complete remission was achieved in all patients with a single course of therapy. Treatment-related toxicity included nausea, vomiting, mucositis, diarrhea, and liver and kidney function abnormalities, and was low in all patients. There were no deaths during induction therapy.
CONCLUSIONS:
We conclude that this combination is well-tolerated in induction of remission in secondary acute myeloid leukemia, and warrants further assessment because of a very good complete remission rate.
 |






